Venlafaxine
 |
|
|---|---|
 |
|
| Systematic (IUPAC) name | |
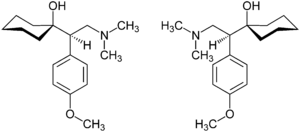
| (RS)-1-[2-dimethylamino-1-(4-methoxyphenyl)-ethyl]cyclohexanol | |
| Identifiers | |
| CAS number | 93413-69-5 |
| ATC code | N06AX16 |
| PubChem | CID 5656 |
| DrugBank | APRD00125 |
| ChemSpider | 56641 |
| Chemical data | |
| Formula | C17H27NO2 |
| Mol. mass | 277.402 g/mol |
| SMILES | eMolecules & PubChem |
| Pharmacokinetic data | |
| Bioavailability | 45% |
| Protein binding | 27% |
| Metabolism | Hepatic |
| Half-life | 5 ± 2 h (parent compound); 11 ± 2 h (active metabolite) |
| Excretion | Renal |
| Therapeutic considerations | |
| Pregnancy cat. | C |
| Legal status | POM (UK) ℞-only (US) |
| Routes | Oral |
| |
|
Venlafaxine (Effexor, Efexor) is an arylalkanolamine serotonin-norepinephrine reuptake inhibitor (SNRI)[1]. It has a similar chemical structure to the opioid derivative tramadol, and has the tertiary amine functional group necessary for µ-opioid receptor recognition (cf. lefetamine), though it is unknown whether it has an opioid agonist effect. It is surprisingly effective in treating depression in heroin and other opioid addicts compared to all other conventional antidepressants.
First introduced by Wyeth in 1993, now marketed by Pfizer, it is licensed for the treatment of major depressive disorder (MDD), as a treatment for generalized anxiety disorder, and comorbid indications in certain anxiety disorders with depression. In 2007, venlafaxine was the sixth most commonly prescribed antidepressant on the U.S. retail market, with 17.2 million prescriptions.[2] In children and adolescents, venlafaxine (like other antidepressants) has a potential to increase suicidal thoughts, attempts and events of self-harm.
Contents |
Indications
Approved
Venlafaxine is used primarily for the treatment of major depression in adults.[3]
Depression
Multiple double blind studies show venlafaxine's effectiveness in treating depression. Venlafaxine has similar efficacy to the tricyclic antidepressants amitriptyline (Elavil) and imipramine, and is better tolerated than amitriptyline. Its efficacy is similar to or better than sertraline (Zoloft) and fluoxetine (Prozac), depending on the criteria and rating scales used. Higher doses of venlafaxine are more effective, and more patients achieved remission or were "very much improved". The efficacy was similar if the number of patients who achieved "response" or were "improved" was considered. A meta-analysis comparing venlafaxine and combined groups of SSRI or tricyclic antidepressants showed venlafaxine's superiority.[4] Judged by the same criteria, venlafaxine was similar in efficacy to the atypical antidepressant bupropion (Wellbutrin); however, the remission rate was significantly lower for venlafaxine.[5] In a double-blind study, patients who did not respond to an SSRI were switched to venlafaxine or citalopram. Similar improvement was observed in both groups.[6]
Off-label/investigational uses
Many doctors are starting to prescribe venlafaxine "off label" for the treatment of diabetic neuropathy (in a similar manner to duloxetine) and migraine prophylaxis (in some people, however, venlafaxine can exacerbate or cause migraines). Studies have shown venlafaxine's effectiveness for these conditions.[7][8] It has also been found to reduce the severity of 'hot flashes' in menopausal women.[9][10]
Substantial weight loss in patients with major depression, generalized anxiety disorder, and social phobia has been noted, but the manufacturer does not recommend use as an anorectic either alone or in combination with phentermine or other amphetamine-like drugs.[3] Venlafaxine hydrochloride is in the phenethylamine class of modern chemicals, which includes amphetamine, methylendioxymethamphetamine (MDMA), and methamphetamine. This chemical structure likely lends to its activating properties; however, some patients find venlafaxine highly sedating, despite its more common stimulatory effects.
Venlafaxine is not approved for the treatment of depressive phases of bipolar disorder; this has some potential danger as venlafaxine can induce mania, mixed states, rapid cycling and/or psychosis in some bipolar patients, particularly if they are not also being treated with a mood stabilizer.[3]
Due to its action on both the serotoninergic and adrenergic systems, venlafaxine is also used as a treatment to reduce episodes of cataplexy, a form of muscle weakness, in patients with the sleep disorder narcolepsy.[11]
Venlafaxine was found in one study to be equal to anafranil (Clomipramine) in the treatment of OCD with fewer side effects.[12]
Due to its tendency to increase blood pressure and its modulative effects on the autonomic nervous system, venlafaxine is often used to treat orthostatic intolerance and postural orthostatic tachycardia syndrome.[13]
Contraindications
Venlafaxine is contraindicated in children and adolescents because it can increase suicidal thoughts, attempts, and self-harm (see Venlafaxine#Suicidality). Furthermore, studies of venlafaxine in these age groups have not established its efficacy or safety.[14] Venlafaxine is not recommended in patients hypersensitive to it, nor should it be taken by anyone who is allergic to the inactive ingredients, which include gelatin, cellulose, ethylcellulose, iron oxide, titanium dioxide and hypromellose. It should never be used with a monoamine oxidase inhibitor (MAOI), as it can cause potentially deadly serotonin syndrome. At least 14 days must pass between the use of venlafaxine and MAO inhibitors. Caution should also be used in those with a seizure disorder.
Glaucoma
Venlafaxine can increase eye pressure, so those with glaucoma may require more frequent eye checks.[3]
Pregnant women
There are few, well-controlled studies of venlafaxine in pregnant women. A study released in May 2010 by the Canadian Medical Association Journal suggests use of venlafaxine doubles the risk of miscarriage.[15] Consequently, venlafaxine should only be used during pregnancy if clearly needed.[3] Prospective studies have not shown any statistically significant congenital malformations.[16] There have, however, been some reports of self-limiting effects on newborn infants.[17] As with other serotonin reuptake inhibitors, these effects are generally short-lived, lasting only 3 to 5 days,[18] and rarely resulting in severe complications.[19] Use of Venlafaxine in pregnancy should be considered on a case-by-case basis. Venlafaxine use during pregnancy increases the risk of spontaneous abortion.[20][21]
Heart disease and hypertension
The FDA asked the manufacturers of all SNRIs to include the risk of persistent pulmonary hypertension (PPHN) in prescribing data as of July 19, 2006. Medications containing venlafaxine caused a mean heart rate increase of 4 bpm in clinical trials, along with a sustained increase in blood pressure in some.
Adverse effects
Suicide
The US Food and Drug Administration body (FDA) requires all antidepressants, including venlafaxine, to carry a black box warning with a generic warning about a possible suicide risk. In addition, the most recent research indicated that patients taking venlafaxine are at increased risk of suicide.
A study conducted in Finland followed more than 15,000 patients for 3.4 years. Venlafaxine increased suicide risk 1.6-fold (statistically significant), as compared to no treatment. At the same time, fluoxetine (Prozac) halved the suicide risk.[22]
In another study, the data on more than 200,000 cases were obtained from the UK general practice research database. The patients taking venlafaxine had significantly higher risk of completed suicide than the ones on fluoxetine (Prozac) (2.8 times) or citalopram (Celexa) (2.4 times). Even after taking into consideration the fact that venlafaxine was generally prescribed for more severe depression, venlafaxine was associated with 1.6-1.7 times more suicides than fluoxetine or citalopram. This difference was no longer statistically significant due to the rarity of completed suicides. However, for the attempted suicides (more frequent event) the 1.2-1.3 times higher risk for venlafaxine still stayed statistically significant after the adjustment.[23]
An analysis of clinical trials by the FDA statisticians showed the incidence of suicidal behaviour among the adults on venlafaxine to be not significantly different from fluoxetine or placebo.[24] A possible explanation for this discrepancy is that suicidal patients are generally excluded from clinical trials, and so clinical trials do not represent the real population of patients.
Venlafaxine is contraindicated in children, adolescents and young adults. According to the FDA analysis of clinical trials[24] venlafaxine caused a statistically significant 5-fold increase in suicidal ideation and behavior in persons younger than 25. In another analysis, venlafaxine was no better than placebo among children (7–11 years old), but improved depression in adolescents (12–17 years old). However, in both groups, hostility and suicidal behavior increased in comparison to those receiving a placebo.[25] In a study involving antidepressants that had failed to produce results in depressed teenagers, teens whose SSRI treatment had failed who were randomly switched to either another SSRI or to venlafaxine showed an increased rate of suicide on venlafaxine. Among teenagers who were suicidal at the beginning of the study, the rate of suicidal attempts and self-harm was significantly higher, by about 60%, after the switch to venlafaxine than after the switch to an SSRI.[26]
Common side effects
NOTE: The percentage of occurrences for each side effect listed comes from clinical trial data provided by Wyeth Pharmaceuticals Inc. The percentages indicate the percentage of people that experienced the side effect in clinical trials.[3]
- Headache (34%)
- Nausea (21-35%)
- Insomnia (15-23%)
- Sexual dysfunction (14-34%)
- Dry mouth (12-16%)
- Dizziness (11-20%)
- Sweating (10-14%)
- Decreased appetite (8-20%)
- Abnormal ejaculation (8-16%)
- Hypertension (4-5%)
- Vivid/abnormal dreams (3-7%)
- Akathisia (agitation) (3-4%)
- Decreased libido (3-9%)
- Increased yawning (3-5%)
- Apathy
- Constipation
- Ongoing irritable bowel syndrome
- Fatigue
- Vertigo
- Orthostatic hypotension (postural drop in blood pressure)
- Impulsive actions
- Electric shock-like sensations also called "brain zaps"
- Increased anxiety at the start of treatment
- Memory loss
- Restless legs syndrome
Less common to rare side effects
Note 'Rare' adverse effects occur in fewer than 1 in 1000 patients.
- Cardiac arrhythmia
- Increased serum cholesterol
- Gas or stomach pain
- Abnormal vision
- Nervousness, agitation or increased anxiety
- Panic attacks
- Depressed feelings
- Suicidal thoughts
- Confusion
- Neuroleptic malignant syndrome
- Tremor
- Drowsiness
- Allergic skin reactions
- External bleeding
- Serious bone marrow damage (thrombocytopenia, agranulocytosis)
- Hepatitis
- Pancreatitis
- Seizure
- Tardive dyskinesia
- Dysphagia (difficulty swallowing)
- Psychosis
- Hair loss
- Hostility
- Activation of mania/hypomania
- Weight loss (of concern when treating patients suffering from anorexia nervosa)
- Weight gain (effect not clear, but of concern when treating people who may have body dysmorphic disorder).
- Homicidal thoughts
- Aggression
- Depersonalization
- Visual hallucinations
- Swollen and/or bleeding gums
- Frequent urination
Dose dependency of adverse events
A comparison of adverse event rates in a fixed-dose study comparing venlafaxine 75, 225, and 375 mg/day with placebo revealed a dose dependency for some of the more common adverse events associated with venlafaxine use. The rule for including events was to enumerate those that occurred at an incidence of 5% or more for at least one of the venlafaxine groups and for which the incidence was at least twice the placebo incidence for at least one venlafaxine group. Tests for potential dose relationships for these events (Cochran-Armitage test, with a criterion of exact 2-sided p-value <=0.05) suggested a dose-dependency for several adverse events in this list, including chills, hypertension, anorexia, nausea, agitation, dizziness, somnolence, tremor, yawning, sweating, and abnormal ejaculation.[3]
Memory loss
In a study of 70 patients that compared the tolerability of venlafaxine at standard doses, ranging from 75 to 300 mg, against relatively high doses (rarely prescribed), ranging from 375 to 600 mg per day, for treating DSM-IV major depressive disorder, "failing memory" was reported in 44% of cases. The severity of venlafaxine-induced memory loss was also noted to increase with dose and length of treatment.[27]
Discontinuation syndrome
In vitro studies revealed venlafaxine has virtually no affinity for opiate, benzodiazepine, or N-methyl-D-aspartic acid (NMDA) receptors. It has no significant CNS stimulant activity in rodents. In primate drug discrimination studies, venlafaxine showed no significant stimulant or depressant abuse liability.[3]
Many patients stopping venlafaxine use experience SSRI discontinuation syndrome, i.e. withdrawal symptoms. This is especially noted if a patient misses a dose, but can also occur when reduction of dosage is gradual. The high risk of discontinuation syndrome symptoms may reflect venlafaxine's short half-life.[28] Missing even a single dose can induce discontinuation effects in some patients.[29] Discontinuation is similar in nature to those of SSRIs such as paroxetine (Paxil or Seroxat). Sudden discontinuation of venlafaxine particularly seemed to cause discontinuation symptoms during the first 3 days in a study of 18 patients.[30] As reported in 2001 by Haddad in the journal Drug Safety, "another strategy to consider is switching to fluoxetine, which may suppress the discontinuation symptoms, but which has little tendency to cause such symptoms itself," and then discontinuing that.[28] Some psychiatrists actually prescribe the singular SSRIs to alleviate the symptoms of venlafaxine withdrawal.
Although many other drugs can cause withdrawal symptoms which are not associated with addiction or dependence, for example, anticonvulsants, beta-blockers, nitrates, diuretics, centrally acting antihypertensives, sympathomimetics, heparin, tamoxifen, dopaminergic agents, antipsychotics, and lithium,[28] addiction or dependence is a more common effect described for drugs that (are thought to, or may) improve mental well-being.[31]
Serotonin syndrome
The development of a potentially life-threatening serotonin syndrome (also more recently classified as "serotonin toxicity")[32] may occur with venlafaxine treatment, particularly with concomitant use of serotonergic drugs (including but not limited to SSRI and SNRI)s, many hallucinogens such as tryptamines and phenethylamines(LSD/LSA, DMT, MDMA, MDPV, mescaline for example), dextromethorphan(DXM)/dextrorphan(DXO), tramadol, tapentadol, meperidine/pethidine and triptans) and with drugs that impair metabolism of serotonin (including MAOIs). Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Venlafaxine-induced serotonin syndrome has also been reported when venlafaxine has been taken in isolation in overdose.[33] An abortive serotonin syndrome state, in which some but not all of the symptoms of the full serotonin syndrome are present, has been reported with venlafaxine at mid-range dosages (150 mg per day)[34] A case of a patient with serotonin syndrome induced by low-dose venlafaxine (37.5 mg per day) has also been reported.[35]
Combined serotonin toxicity and SSRI discontinuation syndrome (SSRI withdrawal)
Venlafaxine may be particularly hazardous to those individuals who are susceptible to both venlafaxine-induced serotonin toxicity (also known as serotonin syndrome) and SSRI discontinuation syndrome. In such cases, individuals who have developed the potentially fatal serotonin toxicity and/or may be at risk of doing so, may find cessation or dose reduction unachievable, placing them at continuing risk. As it is not possible to determine which patients are likely to develop the most severe symptoms of the discontinuation syndrome before cessation or dose reduction is attempted, this dual risk requires that all patients are closely monitored during any increase in dosage (when the patient is most at risk of developing serotonin toxicity)[36] and that such increases are carried out in the smallest incremental steps possible. Additionally, patients who recommence venlafaxine or revert to a higher dosage following a failed attempt to discontinue the drug or reduce dosage are another group with an increased risk of developing serotonin toxicity.[31]
Available forms


Effexor is distributed in pentagon-shaped, peach-colored tablets of 25 mg, 37.5 mg, 50 mg, 75 mg, and 100 mg. There is also an extended-release version distributed in capsules of 37.5 mg (gray/peach), 75 mg (peach), and 150 mg (brownish red).
Venlafaxine extended release (XR)
Venlafaxine extended release is chemically the same as normal venlafaxine. The extended release version (sometimes referred to as controlled release) controls the release of the drug into the gastrointestinal tract over a longer period than normal venlafaxine. This results in a lower peak plasma concentration. Studies have shown that the extended release formula has a lower incidence of patients suffering from nausea as a side effect, resulting in a lower number of patients stopping their treatment due to nausea.[37] In Australia, New Zealand and Switzerland, Wyeth sells their venlafaxine XR tablets under the name "Efexor-XR" (note the spelling with one 'f', rather than "Effexor-XR"). In Brazil, Medley sells a venlafaxine XR capsule under the brand name Alenthus XR. In September 2008, Osmotica Pharmaceuticals began marketing venlafaxine extended release tablets in the United States to compete with Wyeth's capsule-form, Effexor-XR. Sales of branded Efexor XR have remained strong, at US$2.7bn.[38] Teva may begin to offer generic Effexor XR in the US on July 1, 2010, per a settlement agreement with Wyeth, but will have to pay Wyeth a portion of the sale price, driving up the cost.[39] Impax may begin to offer generic Effexor XR in the US on July 1, 2011, per a settlement agreement with Wyeth, but, like Teva, will have to pay Wyeth a portion of the sale price.[40]
Generic
Generic venlafaxine is available in the United States as of August 2006 and in Canada as of December 2006 due to patent expiry. Generic forms of the extended-release version have been available in Canada as of January 2007 and currently include Co Venlafaxine XR (Cobalt Pharmaceuticals Inc.), Gen-Venlafaxine XR (Genpharm), Riva-Venlafaxine XR (Laboratoire Riva Inc.), Novo Venlafaxine XR (Novopharm Limited), PMS-Venlafaxine XR (Pharmascience Inc.), Ratio-Venlafaxine XR (ratiopharm), Viepax (in Israel) and Sandoz Venlafaxine XR (Sandoz Canada Inc.). Generic versions of both drug forms are available now in India. Generic versions are also available in the UK such as Vaxalin manufactured by RatioPharm GmbH.[41]
Overdose
Most patients overdosing with venlafaxine develop only mild symptoms. However, severe toxicity is reported, with the most common symptoms being CNS depression, serotonin toxicity, seizure, or cardiac conduction abnormalities.[42] Venlafaxine's toxicity appears to be higher than other SSRIs, with a fatal toxic dose closer to that of the tricyclic antidepressants than the SSRIs. Doses of 900 mg or more are likely to cause moderate toxicity.[43] Deaths have been reported following very large doses.[44][45] Plasma venlafaxine concentrations in overdose survivors have ranged from 6–24 mg/l, while postmortem blood levels in fatalities are often in the 10–90 mg/l range.[46]
On May 31, 2006, The Medicines and Healthcare Products Regulatory Agency (MHRA) UK has concluded its review into all the latest safety evidence relating to venlafaxine, and particularly looked at the risks associated with overdose. The advice is: the need for specialist supervision in those severely depressed or hospitalized patients who need doses 300 mg or more; cardiac contraindications are more targeted towards high risk groups; patients with uncontrolled hypertension should not take venlafaxine, and blood pressure monitoring is recommended for all patients; and updated advice on possible drug interactions.[47]
On 17 October 2006, Wyeth and the FDA notified healthcare professionals of revisions to the Overdosage/Human Experience section of the prescribing information for Effexor (venlafaxine), indicated for treatment of major depressive disorder. In postmarketing experience, there have been reports of overdose with venlafaxine, occurring predominantly in combination with alcohol and/or other drugs. Published retrospective studies report that venlafaxine overdosage may be associated with an increased risk of fatal outcome compared to that observed with SSRI antidepressant products, but lower than that for tricyclic antidepressants. Healthcare professionals are advised to prescribe Effexor and Effexor XR in the smallest quantity of capsules consistent with good patient management to reduce the risk of overdose.[48]
A report in the British Medical Journal in 2002 by Dr. Nicholas Buckley and colleagues at the Department of Clinical Pharmacology and Toxicology, Canberra Hospital, Australia studying fatal toxicity index (deaths per million prescriptions), found that venlafaxine's fatal toxicity is higher than that of other serotoninergic antidepressants, but it is similar to that of some of the less toxic tricyclic antidepressants. Overall, they found serious toxicity could occur following venlafaxine overdose with reports of deaths, arrythmias, and seizures. They did, however, state that this type of data is open to criticism, pointing out that mortality data may be influenced by previous literature and that "less toxic" drugs may be preferentially prescribed to patients at higher risk of poisoning and suicide, but they are also less likely to be listed as the sole cause of death from overdose. It also assumes that drugs are taken in overdose with similar frequency and in similar amounts. They suggested "clinicians need to consider whether factors in their patients reduce or compensate for this risk before prescribing venlafaxine."[49]
The 27 February 2007 Vancouver Sun reported the BC Drug and Poison Information Centre has alerted doctors that the drug poses a significant risk of death from overdose, saying that venlafaxine "appears more toxic than it was originally hoped".[50] A doctor from the Department of Pharmacy Services College of Pharmacy, Medical University of South Carolina, Charleston, South Carolina, reported on the death of a 39-year-old patient with a 30 g overdose.[44] To put this into perspective, a patient would have to take over 66 of the infrequently prescribed 450 mg high dosage pills, or 400 of the commonly prescribed 75 mg pills.
Management of overdose
There is no specific antidote for venlafaxine, and management is generally supportive, providing treatment for the immediate symptoms. Administration of activated charcoal can prevent absorption of the drug. Monitoring of cardiac rhythm and vital signs is indicated. Seizures are managed with benzodiazepines or other anticonvulsants. Forced diuresis, hemodialysis, exchange transfusion, or hemoperfusion are unlikely to be of benefit in hastening the removal of venlafaxine, due to the drug's high volume of distribution.[51]
Mechanism of action
Venlafaxine is a bicyclic antidepressant, and is usually categorized as a serotonin-norepinephrine reuptake inhibitor (SNRI), but it has been referred to as a serotonin-norepinephrine-dopamine reuptake inhibitor.[52][53] It works by blocking the transporter "reuptake" proteins for key neurotransmitters affecting mood, thereby leaving more active neurotransmitters in the synapse. The neurotransmitters affected are serotonin (5-hydroxytryptamine) and norepinephrine (noradrenaline). Additionally, in high doses it weakly inhibits the reuptake of dopamine,[54] with recent evidence showing that the norepinephrine transporter also transports some dopamine as well, implying that SNRIs may also increase dopamine transmission. This is because SNRIs work by inhibiting reuptake, i.e. preventing the serotonin and norepinephrine transporters from taking their respective neurotransmitters back to their storage vesicles for later use. If the norepinephrine transporter normally recycles some dopamine too, then SNRIs will also enhance dopaminergic transmission. However, while concurrent increase in dopamine (particularly in the prefrontal cortex) is likely to occur[55], the antidepressant effects of any drug are believed to result largely from the modulation of serotonin and norepinephrine; dopamine is thought to play a comparatively small role in depression[56].
Pharmacokinetics
Venlafaxine is well absorbed, with at least 92% of an oral dose being absorbed into systemic circulation. It is extensively metabolized in the liver via the CYP2D6 isoenzyme to desvenlafaxine (O-desmethylvenlafaxine), which is just as potent a serotonin-norepinephrine reuptake inhibitor as the parent compound, meaning that the differences in metabolism between extensive and poor metabolizers are not clinically important in terms of efficacy. Side effects, however, are reported to be more severe in CYP2D6 poor metabolizers.[57] Steady-state concentrations of venlafaxine and its metabolite are attained in the blood within 3 days. Therapeutic effects are usually achieved within 3 to 4 weeks. No accumulation of venlafaxine has been observed during chronic administration in healthy subjects. The primary route of excretion of venlafaxine and its metabolites is via the kidneys.[3] The half-life of venlafaxine is relatively short, and, therefore, patients are directed to adhere to a strict medication routine, avoiding missing a dose. Even a single missed dose can result in the withdrawal symptoms.[29]
Carriers of the (T;T) allele of rs2032583 [58] SNP in the ABCB1 gene are seven times less likely to respond to venlafaxine treatment. This genetic variant is present in about two-thirds of people of European descent and 80% to 90% of East Asians.
Drug interactions
Venlafaxine should be taken with caution when using St John's wort.[59] Venlafaxine may lower the seizure threshold, and coadministration with other drugs that lower the seizure threshold such as bupropion and tramadol should be done with caution and at low doses.[60]
There have been false positive phencyclidine (PCP) results caused by venlafaxine, with certain on-site routine urine-based drug tests.[61][62]
Although the synergistic effects may not be as bad as with other antidepressants, it is still not recommended to take venlafaxine with alcohol.[63]
Physical/chemical properties
The chemical structure of venlafaxine is designated (R/S)-1-[2-(dimethylamino)-1-(4 methoxyphenyl)ethyl] cyclohexanol hydrochloride or (±)-1-[a [a- (dimethylamino)methyl] p-methoxybenzyl] cyclohexanol hydrochloride, and it has the empirical formula of C17H27NO2. It is a white to off-white crystalline solid. Venlafaxine is structurally and pharmacologically related to the atypical opioid analgesic tramadol, and more distantly the newly-released opioid nucynta(Tapentadol), but not to any of the conventional antidepressant drugs, including tricyclic antidepressants, SSRIs, MAOIs, or reversible inhibitors of monoamine oxidase A (RIMA).[43]
See also
- Desvenlafaxine
Notes
- ↑ Yardley JP, Husbands GE, Stack G, Butch J, Bicksler J, Moyer JA, Muth EA, Andree T, Fletcher H 3rd, James MN, et al. 2-Phenyl-2-(1-hydroxycycloalkyl)ethylamine derivatives: synthesis and antidepressant activity. J Med Chem. 1990 Oct;33(10):2899-905. doi:10.1021/jm00172a035 PMID 1976813
- ↑ The number of prescriptions was calculated as the total of prescriptions for the corresponding generic and brand-name drugs using data from the charts for generic and brand-name drugs. "Top 200 generic drugs by units in 2007.". Drug Topics, Feb 18, 2008. http://drugtopics.modernmedicine.com/drugtopics/Top200Drugs/ArticleStandard/article/detail/491194. Retrieved 2008-10-23. "Top 200 brand drugs by units in 2007.". Drug Topics, Feb 18, 2008. http://drugtopics.modernmedicine.com/drugtopics/PharmacyFactsAndFigures/ArticleStandard/article/detail/491210. Retrieved 2008-10-23.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 "Effexor Medicines Data Sheet". Wyeth Pharmaceuticals Inc. 2006. http://www.wyeth.com/content/showlabeling.asp?id=99. Retrieved 17 September 2006.
- ↑ Golden RN, Nicholas L (2000). "Antidepressant efficacy of venlafaxine". Depression and anxiety 12 Suppl 1: 45–9. doi:10.1002/1520-6394(2000)12:1 (inactive 2010-07-26). PMID 11098413.
- ↑ Thase ME, Clayton AH, Haight BR, Thompson AH, Modell JG, Johnston JA (2006). "A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability". Journal of clinical psychopharmacology 26 (5): 482–8. doi:10.1097/01.jcp.0000239790.83707.ab. PMID 16974189.
- ↑ Lenox-Smith AJ, Jiang Q (2008). "Venlafaxine extended release versus citalopram in patients with depression unresponsive to a selective serotonin reuptake inhibitor". Int Clin Psychopharmacol 23 (3): 113–9. doi:10.1097/YIC.0b013e3282f424c2. PMID 18408525.
- ↑ Rowbotham M, Goli V, Kunz N, Lei D (2004). "Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study". Pain 110 (3): 697–706. doi:10.1016/j.pain.2004.05.010. PMID 15288411.
- ↑ Ozyalcin S, Talu G, Kiziltan E, Yucel B, Ertas M, Disci R (2005). "The efficacy and safety of venlafaxine in the prophylaxis of migraine". Headache 45 (2): 144–52. doi:10.1111/j.1526-4610.2005.05029.x. PMID 15705120.
- ↑ Mayo Clinic staff (2005). "Beyond hormone therapy: Other medicines may help". Hot flashes: Ease the discomfort of menopause. Mayo Clinic. http://www.mayoclinic.com/invoke.cfm?id=HQ01409. Retrieved 19 August 2005.
- ↑ Schober C, Ansani N (2003). "Venlafaxine hydrochloride for the treatment of hot flashes". Ann Pharmacother 37 (11): 1703–7. doi:10.1345/aph.1C483. PMID 14565812.
- ↑ "Medications". Stanford University School of Medicine, Center for Narcolepsy. Revised 02/07/2003. http://med.stanford.edu/school/Psychiatry/narcolepsy/medications.html. Retrieved 2007-09-03.
- ↑ Albert U, Aguglia E, Maina G, Bogetto F (November 2002). "Venlafaxine versus clomipramine in the treatment of obsessive-compulsive disorder: a preliminary single-blind, 12-week, controlled study" (PDF). J Clin Psychiatry 63 (11): 1004–9. PMID 12444814. http://www.psychiatrist.com/privatepdf/2002/v63n11/v63n1108.pdf.
- ↑ Hain T (Revised 12/30/2007). "Orthostatic Hypotension". www.dizziness-and-balance.com. http://www.dizziness-and-balance.com/disorders/medical/orthostatic.html. Retrieved 2008-03-29.
- ↑ Courtney D (2004). "Selective serotonin reuptake inhibitor and venlafaxine use in children and adolescents with major depressive disorder: a systematic review of published randomized controlled trials". Can J Psychiatry 49 (8): 557–63. PMID 15453105.
- ↑ "Use of antidepressants during pregnancy and the risk of spontaneous abortion", Canadian Medical Association Journal
- ↑ Gentile S (2005). "The safety of newer antidepressants in pregnancy and breastfeeding". Drug Saf 28 (2): 137–52. doi:10.2165/00002018-200528020-00005. PMID 15691224.
- ↑ de Moor R, Mourad L, ter Haar J, Egberts A (2003). "[Withdrawal symptoms in a neonate following exposure to venlafaxine during pregnancy]". Ned Tijdschr Geneeskd 147 (28): 1370–2. PMID 12892015.
- ↑ Ferreira E, Carceller AM, Agogué C, Martin BZ, St-André M, Francoeur D, Bérard A (2007). "[Effects of selective serotonin reuptake inhibitors and venlafaxine during pregnancy in term and preterm neonates]". Pediatrics 119 (1): 52–9. doi:10.1542/peds.2006-2133. PMID 17200271.
- ↑ Moses-Kolko EL, Bogen D, Perel J, Bregar A, Uhl K, Levin B, Wisner KL (2005). "[Neonatal signs after late in utero exposure to serotonin reuptake inhibitors: Literature review and implications for clinical applications]". JAMA 293 (19): 2372–83. doi:10.1001/jama.293.19.2372. PMID 15900008.
- ↑ PMID 19863482 (PubMed)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ PMID 20513781 (PubMed)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ Tiihonen J, Lönnqvist J, Wahlbeck K, Klaukka T, Tanskanen A, Haukka J (2006). "Antidepressants and the risk of suicide, attempted suicide, and overall mortality in a nationwide cohort". Arch. Gen. Psychiatry 63 (12): 1358–67. doi:10.1001/archpsyc.63.12.1358. PMID 17146010.
- ↑ Rubino A, Roskell N, Tennis P, Mines D, Weich S, Andrews E (2007). "Risk of suicide during treatment with venlafaxine, citalopram, fluoxetine, and dothiepin: retrospective cohort study". BMJ 334 (7587): 242. doi:10.1136/bmj.39041.445104.BE. PMID 17164297.
- ↑ 24.0 24.1 "Overview for December 13 Meeting of Psychopharmacologic Drugs Advisory Committee" (PDF). November 16, 2006. http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Retrieved 2007-06-20.
- ↑ Emslie GJ, Findling RL, Yeung PP, Kunz NR, Li Y (2007). "Venlafaxine ER for the treatment of pediatric subjects with depression: results of two placebo-controlled trials". Journal of the American Academy of Child and Adolescent Psychiatry 46 (4): 479–88. doi:10.1097/chi.0b013e31802f5f03. PMID 17420682.
- ↑ Brent DA, Emslie GJ, Clarke GN, et al. (April 2009). "Predictors of spontaneous and systematically assessed suicidal adverse events in the treatment of SSRI-resistant depression in adolescents (TORDIA) study". Am J Psychiatry 166 (4): 418–26. doi:10.1176/appi.ajp.2008.08070976. PMID 19223438.
- ↑ Harrison CL, Ferrier N, Young AH (June 2004). "Tolerability of high-dose venlafaxine in depressed patients". J. Psychopharmacol. (Oxford) 18 (2): 200–4. doi:10.1177/0269881104042621. PMID 15260908.
- ↑ 28.0 28.1 28.2 Haddad PM (2001). "Antidepressant discontinuation syndromes". Drug Saf 24 (3): 183–97. doi:10.2165/00002018-200124030-00003. PMID 11347722.
- ↑ 29.0 29.1 Parker G, Blennerhassett J (1998). "Withdrawal reactions associated with venlafaxine". Aust N Z J Psychiatry 32 (2): 291–4. doi:10.3109/00048679809062742. PMID 9588310.
- ↑ Fava M, Mulroy R, Alpert J, Nierenberg A, Rosenbaum J (1997). "Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine". Am J Psychiatry 154 (12): 1760–2. PMID 9396960.
- ↑ 31.0 31.1 Double D (1997). "Prescribing antidepressants in general practice. People may become psychologically dependent on antidepressants". BMJ 314 (7083): 829. PMID 9081020.
- ↑ Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM (September 2003). "The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity". QJM 96 (9): 635–42. doi:10.1093/qjmed/hcg109. PMID 12925718. http://www.qjmed.oxfordjournals.org/cgi/content/full/96/9/635.
- ↑ Kolecki P (1997). "Isolated venlafaxine-induced serotonin syndrome". J Emerg Med 15 (4): 491–3. doi:10.1016/S0736-4679(97)00078-4. PMID 9279702.
- ↑ Ebert D. et al.. "Hallucinations as a side effect of venlafaxine treatment". Psychiatry On-line. http://www.priory.com/psych/venhall.htm. Retrieved 2008-06-17.
- ↑ Pan JJ, Shen WW (February 2003). "Serotonin syndrome induced by low-dose venlafaxine". Ann Pharmacother 37 (2): 209–11. doi:10.1345/aph.1C021. PMID 12549949.
- ↑ Venlafaxine (marketed as Effexor) FDA Alert: SSRIs/SNRI/Triptan and Serotonin Syndrome [issued 7/2006]
- ↑ DeVane CL. (2003). "Immediate-release versus controlled-release formulations: pharmacokinetics of newer antidepressants in relation to nausea". J Clin Psychiatry 64 (Suppl 18): 14–9. PMID 14700450.
- ↑ Details for Effexor XR
- ↑ http://www.wyeth.com/irj/servlet/prt/portal/prtroot/com.sap.km.cm.docs//wyeth_xml/home/news/announcements/1153395074748.pdf (Archived by WebCite® at http://www.webcitation.org/5pXQuFykU) p. 3, 4
- ↑ httphttp://www.wyeth.com/irj/portal/news/archive?nav=display&navTo=/wyeth_html/home/news/pressreleases/2008/1216240549738.html
- ↑ [1]
- ↑ Blythe D, Hackett L (1999). "Cardiovascular and neurological toxicity of venlafaxine". Hum Exp Toxicol 18 (5): 309–13. doi:10.1191/096032799678840165. PMID 10372752.
- ↑ 43.0 43.1 Whyte I, Dawson A, Buckley N (2003). "Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants". QJM 96 (5): 369–74. doi:10.1093/qjmed/hcg062. PMID 12702786.
- ↑ 44.0 44.1 Mazur J, Doty J, Krygiel A (2003). "Fatality related to a 30-g venlafaxine overdose". Pharmacotherapy 23 (12): 1668–72. doi:10.1592/phco.23.15.1668.31951. PMID 14695048.
- ↑ Banham N (1998). "Fatal venlafaxine overdose". Med J Aust 169 (8): 445, 448. PMID 9830400.
- ↑ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 1634-1637.
- ↑ MHRA UK (31 May 2006). "Updated product information for venlafaxine". Safeguarding public health 120: 778. doi:10.1016/j.puhe.2006.03.006.
- ↑ "Wyeth Letter to Health Care Providers". Wyeth Pharmaceuticals Inc. 2006. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm150546.htm. Retrieved 2009-08-06.
- ↑ Buckley N, McManus P (2002). "Fatal toxicity of serotoninergic and other antidepressant drugs: analysis of United Kingdom mortality data". BMJ 325 (7376): 1332–3. doi:10.1136/bmj.325.7376.1332. PMID 12468481.
- ↑ Fayerman, Pamela (February 27, 2007). "Warning issued over drug". Vancouver Sun. http://www.canada.com/vancouversun/news/story.html?id=83f35b4e-ac13-4c09-b8de-44d16750b70b&k=58837. Retrieved 2007-06-02.
- ↑ Hanekamp B, Zijlstra J, Tulleken J, Ligtenberg J, van der Werf T, Hofstra L (2005). "Serotonin syndrome and rhabdomyolysis in venlafaxine poisoning: a case report". Neth J Med 63 (8): 316–8. PMID 16186642.
- ↑ [No Authors listed]. "Acute Effectiveness of Additional Drugs to the Standard Treatment of Depression". ClinicalTrials.gov. http://www.clinicaltrials.gov/ct/show/NCT00001483. Retrieved 23 June 2005.
- ↑ Goeringer K, McIntyre I, Drummer O (2001). "Postmortem tissue concentrations of venlafaxine". Forensic Sci Int 121 (1-2): 70–5. doi:10.1016/S0379-0738(01)00455-8. PMID 11516890.
- ↑ Wellington K, Perry C (2001). "Venlafaxine extended-release: a review of its use in the management of major depression". CNS Drugs 15 (8): 643–69. doi:10.2165/00023210-200115080-00007. PMID 11524036.
- ↑ http://stahlonline.cambridge.org/prescribers_drug.jsf?page=0521683505c95_p539-544.html.therapeutics&name=Venlafaxine&title=Therapeutics
- ↑ Delgado, P.L., & Moreno, F.A. (2000). Role of norepinephrine in depression. Journal of Clinical Psychiatry, 61, 5-12.
- ↑ Shams ME et al. (2006). "CYP2D6 polymorphism and clinical effect of the antidepressant venlafaxine". J Clin Pharm Ther 31 (5): 493–502. doi:10.1111/j.1365-2710.2006.00763.x. PMID 16958828.
- ↑ SNPedia
- ↑ Karch, Amy (2006). 2006 Lippincott's Nursing Drug Guide. Philadephia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokyo: Lippincott Williams & Wilkins. ISBN 1-58255-436-6.
- ↑ Thundiyil JG, Kearney TE, Olson KR (March 2007). "Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System". J Med Toxicol 3 (1): 15–9. doi:10.1007/BF03161033. PMID 18072153.
- ↑ Santos PM, López-García P, Navarro JS, Fernández AS, Sádaba B, Vidal JP (February 2007). "False positive phencyclidine results caused by venlafaxine". Am J Psychiatry 164 (2): 349. doi:10.1176/appi.ajp.164.2.349. PMID 17267806. http://ajp.psychiatryonline.org/cgi/content/full/164/2/349.
- ↑ Sena SF, Kazimi S, Wu AH (2002). "False-positive phencyclidine immunoassay results caused by venlafaxine and O-desmethylvenlafaxine". Clin. Chem. 48 (4): 676–7. PMID 11901076. http://clinchem.org/cgi/content/full/48/4/676.
- ↑ http://www.nhs.uk/chq/Pages/863.aspx?CategoryID=73&SubCategoryID=103
External links
Drug information
- U.S. Food and Drug Administration information on Effexor
- Efexor patient information leaflet Efexor patient information leaflet
- Effexor XR prescribing information for healthcare professionals (pdf) (USA only)
- Detailed Patient/Parent Information on Effexor
- List of international brand names for Venlafaxine
- U.S. National Library of Medicine: Drug Information Portal - Venlafaxine
Diagnostic Tools
Patient experiences
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||